TechBuzz profiles Alison Smart’s campaign to preserve Levemir, the discontinued insulin detemir that some patients uniquely need, through stories from Michela Belluta, Kirill Zenchenko, Jaime Losinski, and Dr. Maisa Feghali, who warn alternatives can be riskier.
Utah State Legislators Todd Weiler, Ray Ward, MD, and Even Vickers, Pharmacist with Alison Smart, Founder of Alliance to Protect Insulin Choice, at the Utah State Capitol
Utah State Legislators Todd Weiler, Ray Ward, MD, and Even Vickers, Pharmacist with Alison Smart, Founder of Alliance to Protect Insulin Choice, at the Utah State Capitol
Salt Lake City, Utah - June 3, 2026
As insulin drug Levemir disappears, patients, parents, and physicians say other basal insulins are not true substitutes. Alison Smart of Bountiful Utah has turned that warning into a coordinated campaign to preserve insulin choice before more families are pushed into riskier workarounds.
A box of insulin sits in a refrigerator in Milan, waiting for Michela Belluta’s next trip home.
Belluta, who lives in the U.S. and was diagnosed with type 1 diabetes as an adult, has found herself doing something that sounds implausible in a modern healthcare system: traveling to Italy and bringing back Levemir because it is the only basal insulin she trusts not to send her into a dangerous low.
“That’s how I keep going with Levemir,” she said. “It’s crazy that we cannot access a medication that is unique. It’s not that we can turn to another brand.”
For Alison Smart, stories like Belluta’s are no longer isolated anecdotes. They are evidence. Over the last year, Smart has emerged as one of the most visible organizers in the fight to preserve access to insulin detemir, sold for years as Levemir. Through her not-for-profit, Alliance to Protect Insulin Choice, she has gathered patient accounts, physician statements, a white paper, and conversations with manufacturers and regulators into something more structured: a case that this is not a matter of preference, but of medical necessity.
And the ask, she says, is not glamorous.
“We want it as simple as possible,” Smart told TechBuzz. “Just give us the liquid in little bottles, in vials.”
That simplicity is part of what makes the story so striking. In an era of continuous glucose monitors, automated insulin delivery, telehealth platforms, AI-assisted drug discovery, and blockbuster metabolic therapies, some patients are fighting for a decades-old insulin because, for them, nothing else works quite the same way.
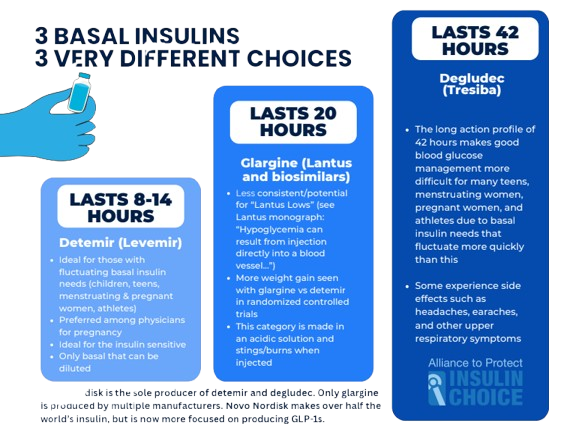
The central argument from Smart’s coalition is straightforward: basal insulin is not interchangeable for everyone. Levemir’s pharmacology, particularly its shorter action profile and flexibility for split dosing, made it uniquely useful for some pregnant women, children, teens, highly insulin-sensitive adults, athletes, and people who do poorly on alternatives like insulin glargine or degludec. Yet as the product has been withdrawn from the U.S. market and becomes harder to source globally, those patients are being told, implicitly or explicitly, to adapt.
For many, “just switch” is not a real plan.
Sarah Newman, Member of Alliance to Protect Insulin Choice and Alison Smart, Founder of Alliance to Protect Insulin Choice
The hidden problem inside the word “insulin”
Part of what has made this fight difficult is that, to most outsiders, insulin sounds like a single category rather than a family of distinct tools.
“People may be familiar with insulin,” said Dr. Maisa Feghali, a maternal-fetal medicine physician and associate professor at the University of Pittsburgh Medical Center, “but very few people have an understanding of all the biosimilar options related to insulin and sort of think of insulin as one single entity.”
That misunderstanding has obscured the scale of the loss. Insulin detemir was the fourth best-selling insulin in the U.S. in 2022, according to ClinCalc. It was also the 127th best-selling drug in the country, with more than 4.8 million prescriptions filled for over 900,000 patients, according to the 2022 Medical Expenditure Panel Survey from the Agency for Healthcare Research and Quality. Consulting firm Close Concerns estimated that detemir generated nearly $650 million in revenue that year.
In other words, Levemir was not an obscure holdover quietly serving a vanishing handful of patients. It remained a major insulin product even as the market, and the industry’s attention, shifted elsewhere.
Feghali sees the consequences most clearly in pregnancy, where insulin needs can shift quickly and the margin for error is narrow.
“We have to extrapolate from alternative agents,” she said, referring to other basal insulins with different pharmacologic profiles, “and then, with some changes and some adjustments, try to emulate the benefit that was more evident to us with the use of detemir.”
That is not how progress is supposed to feel.
“It feels like a scramble when we shouldn’t be,” Feghali said.
In pregnancy, she said, patients are already being told that tight control matters early and matters a lot. At the same time, they are being forced into medication changes and troubleshooting cycles they did not ask for.
“On one end, they’re receiving this message of needing tight control and needing early control,” Feghali said. “And on the other end, we are throwing all these curve balls and changes at them.”
Dr. Dorothy Fink, Deputy Assistant Secretary for Women's Health and Director of the Office on Women's Health in the Office of the Assistant Secretary for Health (OASH) at the U.S. Department of Health and Human Services, with Alison Smart, Founder of Alliance to Protect Insulin Choice
Smart’s coalition has collected comments from women who relied on Levemir through pregnancy and now fear what comes next. “I’m currently pregnant with twins,” one patient wrote, “and with the constantly changing insulin needs that come along with pregnancy, I would be absolutely lost without the flexibility of Levemir.” Another said the insulin helped her achieve healthy A1Cs during one pregnancy and that she is “desperate” to keep access to reproduce those results in another.
For Feghali, this is not an argument against innovation. It is an argument against innovation that erases useful variation.
“There is less enthusiasm and support toward the less shiny kind of old insulin varieties and a lot more excitement about the shiny new technology that’s being developed,” she said. “What we need to do is just maintain the variability, maintain the options that are available so that we are providing each single patient with the type of insulin that is most effective and most in line with their physiologic needs.”
Patients pushed into workarounds
Belluta’s workaround is international. Others are domestic, but no less precarious.
Kirill Zenchenko, a father in western Massachusetts, says his nine-year-old son Pax was diagnosed with type 1 diabetes at two and a half. The family used an insulin pump early on, but as his son remained small, the hardware became its own problem.
“The pump chewed up his body,” Zenchenko said.
Site rotation became harder, absorption became less reliable, and eventually the family pulled him out of preschool because his glucose was so difficult to control.
Then they switched to Levemir.
Pax’s A1C improved, Zenchenko said, dropping from the mid-to-low sixes into the mid-to-low fives. Just as important, the family gained flexibility. His son’s daytime and nighttime basal needs were nowhere near the same.
“His daytime needs are three times his nighttime needs right now,” Zenchenko said.
That is the sort of detail that tends to disappear in abstract discussions of “alternative options.” But for families managing type 1 diabetes around the clock, it is the whole point. The wrong basal profile does not just make numbers messier. It invades sleep, school, work, and emotional stability.
“One of the beautiful things of good T1D management is sleep,” Zenchenko said. “If you can have sleep, your whole day is a lot better.”
Smart hears versions of that line often. For families who have already fought hard to reach stability, the disappearance of a working insulin feels like being thrown backwards.
“When you get type 1 diabetes under control and you have things in this stable place,” she said, “to be thrown back into a state of instability is frightening.”
Alison Smart, Founder of Alliance to Protect Insulin Choice, and her daughter, Ruby, with Blake Moore, Republican congressman representing Utah's 1st District in the U.S. House of Representatives
Jaime Losinski, a Florida mother, described that fear in even starker terms. Her teenage son, now almost 17, has been on Levemir for years after bad experiences with both glargine and degludec. On Tresiba, she said, “I was just lost in the sauce for 48 hours.” On Lantus, he complained that injections burned, and she remembers sudden lows that seemed to come “out of nowhere.”
Levemir, by contrast, has been manageable because it tracks his day-night physiology more closely.
“Never has day and night been the same,” Losinski said. “Never have they even been close.”
Today, she said, “He’s currently on 88 units in the morning and 39 at night.”
Those numbers are dramatic, but they capture why so many patients and parents keep coming back to split dosing. Losinski is now rationing what remains of her family’s Levemir supply and trying to imagine what happens when it runs out.
“How I would dose him with Lantus now, I don’t know,” she said.
Her son is also exactly the sort of patient who exposes the weakness of another common fallback: the insulin pump. He plays baseball competitively, is self-conscious about visible devices, and already tolerates a CGM only on his own terms.
“He does not want another thing attached,” Losinski said.
Smart is careful not to paint pumps as bad technology. Many people do well on them. But she argues that “just use a pump” has become a reflexive answer to a more complex problem.
“It feels like a bandaid,” Smart said. “It’s not a complete solution because you still need the backup for a pump.”
That matters in power outages, during pump failures, around surgeries and medical procedures, and for patients who simply cannot or will not use another wearable device.
The same pattern appears in other families Smart has heard from. One parent described a son diagnosed at 11 months old who needed Levemir diluted to tiny doses of 0.1 units after “frequent scary lows” early in diagnosis. “This turned out to be a game changer and we’ve never looked back,” the parent wrote. Another teenager put it even more simply: “I’m 15 and my body needs twice the amount of insulin during the day than it does at night. Levemir is the only insulin that can safely match what my body needs.”
These are edge cases only if you choose to define them that way. In practice, they are the kinds of differences diabetes care has to accommodate.
The market logic, and the human cost
From the patient side, the pattern looks brutal: something works, the market shifts, and the burden of adaptation falls onto the person with the chronic disease.
Belluta remembers the alternatives not as minor inconveniences but as emergencies.
“Lantus gave me a very bad low and I ended up in the ER,” she said.
Years later, when she tried Tresiba, she said, “I had another really bad hypo and I ended up in the ER again.”
That history is why her next switch feels less like an experiment than a threat.
“If you change the medication,” she said, “everything is going back to square one, as if it’s your first day of being diabetic.”
Feghali hears a similar frustration in pregnancy patients, who often conclude that they are being left behind because the medication no longer fits the commercial priorities of the companies that once sold it.
“There’s a feeling that patients are being left behind because of profit measures or market measures that the companies are trying to follow,” she said.
Smart’s account of the market shift is blunt but not ideological. When newer, patent-protected insulin products arrived, sales attention moved with them. Then came the explosion of GLP-1 demand and a broader industry pivot toward higher-growth product lines. None of that means other technologies are bad. It does mean older therapies can become vulnerable even when they still solve a real problem.
That tension between innovation and continuity is what makes this more than a niche diabetes story. It is a systems story. Healthcare markets are good at rewarding what is new, scalable, and highly profitable. They are much worse at preserving “legacy” therapies that remain indispensable for smaller but still substantial patient populations.
Feghali worries the result will not stop with one insulin.
“As there’s more and more focus towards productivity and reimbursement,” she said, “we’ll lose a lot more options when it comes to insulin, and we’ll be limited with the options that we have to take care of patients with individual needs.”
Alison Smart’s practical campaign
What Smart has done well is turn a diffuse sense of panic into a policy argument.
Her coalition’s white paper lays out the case that insulin detemir remains medically necessary for specific populations, including pregnant women, children and adolescents, patients with narrow therapeutic windows, and people who cannot tolerate glargine, degludec, or pump therapy. It argues that other basal insulins do not fully replicate detemir’s shorter action profile, dosing flexibility, and patient-specific tolerability. And it makes a practical point: if manufacturers are willing to produce detemir, what they need is a clear regulatory pathway.
That is where Smart has focused much of her energy, asking the FDA to place detemir on the Drug Shortage List.
“To fill the definition, it needs to show proven harm without that drug and there needs to be not enough of that drug to meet the demand,” she said of the shortage framework she believes applies here. “So it absolutely meets both of those requirements.”
The broader ask is not for a miracle. It is for FDA and HHS to clarify a path that would allow another manufacturer to produce insulin detemir while maintaining safety and efficacy standards. In Smart’s view, that would protect patient choice, preserve resilience in the insulin supply, and keep vulnerable populations from becoming collateral damage in an industry portfolio shift.
Bobby Mukamala, MD, President of American Medical Association in Washington, DC, with Alison Smart, Founder of Alliance to Protect Insulin Choice, at an HHS announcement in the Hubert H. Humphry Building
Feghali agrees that the answer should not be to wait passively while options disappear.
“There should be support from the point of view of the regulators for generic availability of things like Levemir,” she said, “that have been proven to be beneficial but may not fit into the long-term market plan.”
In the meantime, patients are doing what patients always do in a brittle system: stockpiling, calling pharmacies, planning around scarcity, and hoping someone with authority notices before the last vial is gone.
That is why Belluta’s parents still keep insulin in their fridge in Italy. It is why Losinski is counting months. It is why Zenchenko is thinking about what it means to lose not just a medication, but the sleep and stability it made possible. And it is why physicians like Feghali are speaking up even as they continue to improvise with less ideal alternatives.
“I don’t want to try to take away from progress in any way,” Feghali said. “But I also don’t think that progress should take away from a lot of the variation that has been proven, especially in specific populations like pregnancy, to be beneficial.”
That may be the cleanest way to understand what Smart and her coalition are fighting for. Not nostalgia. Not resistance to new technology. Just the preservation of an option that still matters.
Or, as Smart put it with characteristic economy: “We’ll be quiet. We’ll leave you all alone. Just give us our insulin.”